Saturday, August 8, 2026
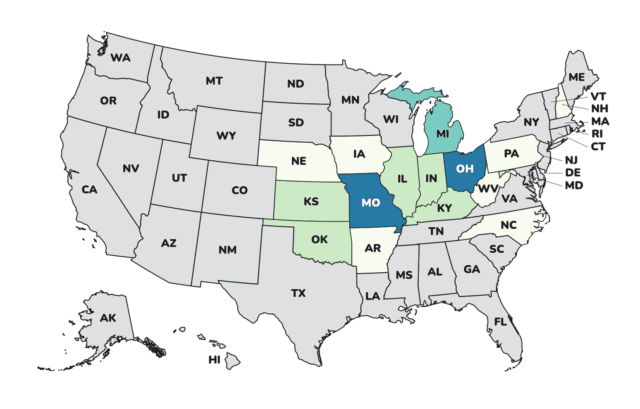
Last Saturday this column was called The Week Cyclospora Stopped Being a Health Story and Became an Accounting One. This week the accounting stopped being the argument. On Monday it was announced that two people died in Michigan. On Tuesday a newspaper announced a federal expansion the government had not. On Wednesday the government’s own count went from 1,947 people in nine states to 6,358 in fifteen, and not one of those additional 4,411 Americans got sick that day. What changed was a definition.
Two people died, and the state said no additional information would be provided. Michigan announced on Monday that both individuals had significant underlying health conditions that may have been impacted by cyclosporiasis and dehydration, that both fell ill before the July 17 recall, and that nothing further would be released. These are the first deaths anywhere in this outbreak. May have been impacted by is contributory language, not a finding on cause of death, and I will not stretch it into one. But I wrote on Monday and will say it again: who the hell cares that they had significant underlying health conditions. Most people who die in a foodborne outbreak do. It kills the very young, the very old and the immune compromised — that is who it has always killed, and the phrase does not make either loss smaller. I have represented families of people who died after eating a salad, and their losses were every bit as significant as anyone else’s. Nor has anyone described how a Cyclospora death gets counted in the first place.
The Washington Post announced the expansion two days before the government did. Lena H. Sun and Rachel Roubein reported Tuesday afternoon that CDC was expanding this outbreak from nine states to fifteen, attributed to three individuals familiar with the investigation, and by 4:13 p.m. Eastern they had named all six additions — Arkansas, Iowa, Missouri, Nebraska, New Hampshire and North Carolina. Every federal page still said nine that afternoon. Sun and Roubein have been right every time; this is about what has happened to the announcement channel for a federal outbreak investigation, and it was the second time in twelve days.
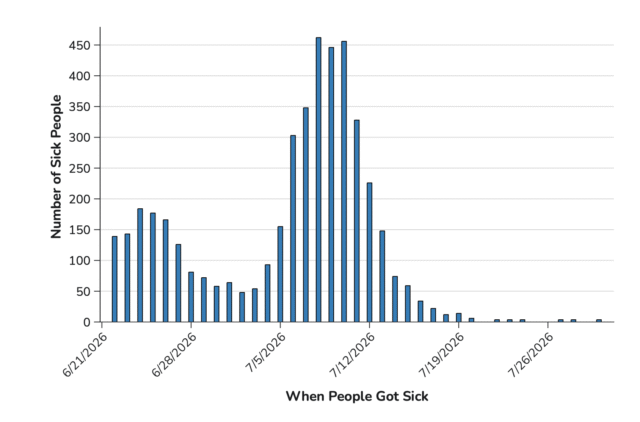
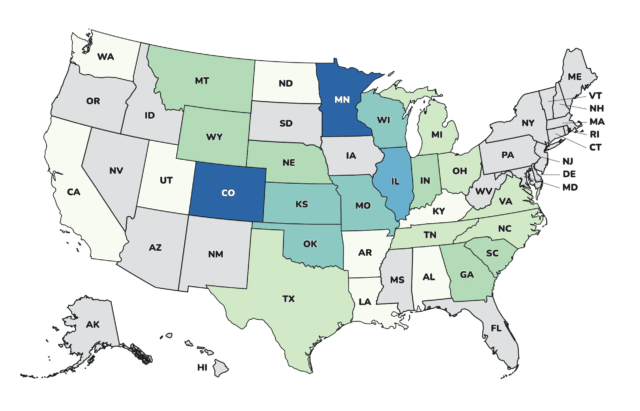
Then the federal count tripled, and nobody new got sick. On Wednesday CDC and FDA both posted it: 6,358 illnesses, fifteen states, 278 hospitalizations, two deaths. The day before, the same outbreak was 1,947 people in nine states. The case definition widened — until Wednesday a person entered by reporting they ate at Taco Bell, and now they can enter by eating at Taco Bell or by eating recalled Taylor Farms lettuce anywhere at all. The change was not announced, not dated, and the earlier series was not republished, so no trend line through it means anything. It is the point I have been making since mid-July. The federal number was never measuring a parasite. It was measuring one restaurant chain.
Taylor Farms says the lettuce shipped June 29. FDA says people started getting sick June 22.The company told the Post the recalled shredded iceberg went out June 29 through July 16, and when the paper asked what had shipped before June 29, it declined to say. CDC puts incubation at two to fourteen days, so a June 22 onset means an exposure at least nine days before the recall window even opens. New Hampshire published its own exposure window, the beginning of June through July 20 — four weeks wider than the company’s at the front, with a street address on it. A recall is a boundary drawn on a calendar. Taylor Farms drew this one and will not say what is on the other side of the line.
And Taylor Farms’ own page now says two different things about where the lettuce went. The company put up a Cyclospora information hub this week: central Mexico sourcing suspended for the season, production there halted since July 18, outside experts commissioned, roughly two thousand of its own samples negative since May, and a concession it spent July arguing around — that epidemiological evidence is a legitimate tool in an outbreak investigation. Read it twice, though. Its recall notice lists twenty-seven states without West Virginia; its own FAQ answers the same question with twenty-eight, West Virginia included. FDA’s advisory has the identical split between two of its sections. West Virginia has been an outbreak state since July 14, Nebraska is on neither list, and nobody has explained how a state joins an outbreak traced to a product the shipping records say never arrived. One line there is worth the whole page: the company says its water sources are tested for indicator organisms. That is generic E. coli — the only numeric criterion in the federal agricultural water rule, and the organism FDA’s own guidance says will not find this parasite. They are doing what the rule asks. The rule asks for the wrong test. CNN spent the week on the pattern behind all of it. Casey Tolan, Yahya Abou-Ghazala, Curt Devine and Kyung Lah counted at least five Cyclospora and E. colioutbreaks tied to the company over the past decade, and Lah put it on television Friday. A former senior FDA official says the company worked hard to keep the agency from naming it in the 2024 McDonald’s onion outbreak. FDA has not inspected the Guanajuato plant since 2019, and this year five of the company’s more than 160,000 Mexican shipments were physically inspected. People eat the evidence. A negative result on what is left in the cooler is not a finding of innocence, and it is no substitute for a name.
Michigan alone now reports more people hospitalized than the entire fifteen-state outbreak.The state finished the week at 12,485 cases with 279 hospitalizations. The federal figure for all fifteen states is 278. The same afternoon it reported that 279, Michigan lifted its bagged-salad advisory. Natasha Bagdasarian, the state’s chief medical executive, said the worst is behind us on the data available today, and was careful to say she meant Michigan. The state is also going from daily to weekly reporting, so the number that has driven this count all summer will now arrive once a week.
Ohio has now reported sixty-four times what it reported in all of last year. The state dashboard passed 4,900 cases, with 3,399 confirmed between July 4 and August 4 alone. Ohio confirmed 76 in all of 2025. Arkansas is at 237 against seven last year, 144 of them in Benton County, against the 41 Arkansans CDC counts in the fifteen-state outbreak. Add every state’s own published number and the floor is 26,755 people, up 5,303 in a week. CDC’s surveillance page reads 10,468 laboratory-confirmed plus 12,255 awaiting confirmation, unmoved since Tuesday. Hold any of those against the 249 cases reported nationally by this point last year.
FDA opened a brand-new Cyclospora investigation the same day it announced the old one had reached 6,358. The agency’s outbreak table now carries seven Cyclospora files and one of them names a food. Reference 1398 was posted August 5 — ten people, no vehicle. Reference 1385 went from 10 to 25, which FDA explains by saying it now includes illnesses with similarities in reported exposures — the agency telling you it has found a common exposure pattern in a file whose food it will not name. Six open files, 178 people, no product.
And I put the argument where people could check it. Thursday night Food Safety News ran fifteen things FDA and CDC could do about this parasite, four of which require no rulemaking, no appropriation and no act of Congress. Friday I wrote about recall readiness, which nobody measures until the week they need it. And earlier a box of t-shirts arrived, every one reading Test Infant Formula for Botulism — a different outbreak, four hospitalized babies, the same problem underneath it.
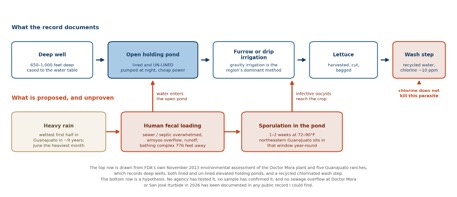
On the blog it was a week of old arguments picking up new proof. Thursday I said what I think of the Secretary’s July 21 assurance that this was under control, and set 2011 beside 2026 — sixty-eight people sick in ten states and CDC called it Restaurant Chain A, against FDA naming Taco Bell in the first sentence of its first advisory this July. Nothing changed in between but the decision to type the name. Friday I gave six reasons the produce trade association is wrong to tell CDC that endemic American water is behind this, the first being that the parasite does not multiply outside a person, so every oocyst in an American lake came out of an American. Marion Nestle told her readers what to do about all of it. And I sat down with KBJR in Duluth on the question I get asked most: when does food poisoning become a lawsuit. It becomes one when nobody will tell a sick family what happened to them.
The jalapeño outbreak got a country, a state and a distributor, but not a grower. CDC posted its Salmonella Javiana outbreak page Wednesday: 345 sick in 27 states, 36 hospitalized, with 177 of 191 interviewed reporting a Mexican-style restaurant and both Chipotle and QDOBA named. The peppers came from Sinaloa by way of Coast Citrus Distributors. The grower was identified by traceback and not named, and the recall carries no lot codes and no consignee list while CDC tells businesses to check whether their peppers are recalled. Javiana is a water organism. Two of the isolates carry antibiotic resistance, one of them multidrug-resistant and nonsusceptible to ciprofloxacin. And look at the sequence. Chipotle switched jalapeño suppliers on July 20 and QDOBA stopped serving them on July 28. FDA opened its traceback on July 22 and named Sinaloa and Coast Citrus on August 5. Two restaurant chains and a Minnesota epidemiologist got there first, and while they did, FDA’s own outbreak table still carried this file at 212 illnesses with no food identified. Three numbers for one outbreak, from one government, in one week. That is the sentence I have been writing about Cyclospora all summer, in a different aisle of the same store.
The recognized record of fresh-pepper Salmonella outbreaks in this country is exactly three, and all three came out of the same place. I put the whole history down this week. In 2008 SalmonellaSaintpaul sickened 1,442 people across 43 states, hospitalized at least 286, and investigators spent the summer wrecking the domestic tomato market before the strain finally turned up on a Mexican-grown jalapeño in a McAllen warehouse and in irrigation water on a farm in Mexico. In 2016 Salmonella Anatum sickened 32 people in nine states, and that one was solved only because FDA’s own laboratory happened to have sequenced an Anaheim pepper months before the outbreak existed. Now 2026. Three outbreaks in eighteen years is not a measure of how often peppers make people sick. It is a measure of how often anybody manages to prove it. After 2008 the Associated Press went through the border records and found chilies were the most-rejected Mexican crop of the preceding year, with Salmonella in eight percent of intercepted shipments. Nobody acted on it. Fresh chilies are grown outdoors in warm climates, irrigated with surface water, harvested by hand and eaten raw, and there is no wash that reliably clears the crevice where the stem meets the fruit. It is the same argument as the lettuce, and it has the same answer at the bottom of it, which is the water.
And the rest of the ledger, because it did not stop for the parasite. FDA’s outbreak table still carries the Midwest Poultry Services shell egg Salmonella Enteritidis outbreak at 98 illnesses and 26 hospitalizations across seventeen states, off a recall of more than nineteen million eggs. A Salmonella Oranienburg cluster sits at 93 with no food named at all. Still open too: the Listeria outbreak in Clover Hill requesón and soft ricotta, twelve sick, ten hospitalized, one dead; the E. coli O145:H28 investigation into GreenWise frozen blueberries sold at Publix; and the infant botulism outbreak behind the Nara Organics formula recall, four babies, all four hospitalized. On Friday USDA pulled 29,628 pounds of Argentine beef and 5,084 pounds of swai from the United Arab Emirates, both of which entered this country without import reinspection. Phyllis Entis has the international roundup at eFoodAlert, as she does every day.
That’s the week — two people dead, a federal count that tripled on a definition instead of an exposure, one state reporting more hospitalizations than the whole outbreak it belongs to, a company that will not say what shipped before the twenty-ninth of June, and a parasite that has made more Americans sick in one summer than the government’s own records show for the previous thirty-four years. And in the same seven days, jalapeños out of Sinaloa put thirty-six people in the hospital across twenty-seven states while the grower stayed anonymous. The season CDC defines runs through August 31. That is twenty-three days. Check back next Saturday.
About Bill Marler
William “Bill” Marler has spent more than thirty years as a food safety lawyer and advocate—work that began with the 1993 Jack in the Box E. coli outbreak and has never really stopped since. In the years that followed, he has represented victims in nearly every major foodborne illness outbreak in the United States. That case, and the movement it launched, is the subject of the book “Poisoned” and the Emmy Award–winning Netflix documentary of the same name. Bill’s work has been profiled in The New Yorker (“A Bug in the System”), the Seattle Times (“30 years after the deadly E. coli outbreak, a Seattle attorney still fights for food safety”), the Washington Post (“He helped make burgers safer. Now he’s fighting food poisoning again”), and many others.
Dozens of times a year, Bill speaks to industry, regulators, and universities across the United States, Canada, Europe, Africa, China, and Australia about a simple idea: outbreaks are preventable. He has testified before Congress on the Food Safety Modernization Act and teaches food safety at institutions including the Harvard T.H. Chan School of Public Health. He writes regularly about food litigation and food safety at Marler Blog, and in 2009 he founded Food Safety News, which he continues to publish.